

By Anton Alers & Anisa Pinatih
The global impact of the COVID-19 pandemic cannot be understated or underestimated. There will be permanent changes in our approach to design and how society responds to the workplace in a post-COVID world. It is also evident that this will not be the last pandemic we will experience and we need to plan accordingly. Healthcare facilities are the obvious building typology where health crises will directly impact design. Hospitals need to adapt and be ready. A proper plan is needed when converting large open spaces—such as conference centres and hotels—to serve as makeshift hospitals or quarantine centres.
PREPARING HOSPITALS: CAPITAL COST WILL PAY OFF
The rate of spread of this pandemic has caught many countries almost by surprise and the sudden demand for intensive care beds and equipment has placed huge demands on the healthcare infrastructure. Flexibility and capacity are key factors in healthcare design. Hospital wards need to be able to convert into isolation units and their air-conditioning systems be able to provide negative pressure to prevent cross-infection. There is a capital cost to providing this additional capability in mechanical ventilation systems, but this cost is less than over-providing permanent intensive care beds when there is no peak demand.
Dedicated circulation routes/zones are often eliminated or minimised due to cost and space planning, especially in the private sector. However, they are necessary to reduce risks of cross contamination in times of health crises. For example, staff should not be expected to commute to and from hospitals in their uniforms and, from a cross-infection perspective, they should change out of their uniforms/scrubs before going out in public. Increased attention is required to protect these essential personnel. Other support facilities also require additional emphasis, such as suitable change rooms, showers, and cafeterias.
For workplaces in general, flexible spaces with the opportunity for hot-desking are likely to be in demand as more of the workforce moves to working from home on a frequent basis.
Accident & Emergency (A&E) Units are required to deal with large numbers of contagious cases, but they also need to deal with normal emergency cases. Expanded emergency departments with space for external triage of suspected contagious cases, decontamination areas and a separate internal A&E zone to isolate contagious cases.
The supply chain has also come under pressure as adequate space is needed for personal protective equipment and apparel for healthcare workers. The economically-driven ‘just in time’ supply chain has been placed under stress and has been shown to be a weak link during the current pandemic. Increased storage space is likely to be demanded in the future by health authorities.
Waste management processes in hospitals usually address contaminated and clinical waste. Items such as surgical masks need to be carefully disposed of in the appropriate clinical waste receptacles. Soiled garments, however, need to be more carefully handled, transported and washed before reuse to avoid cross-contamination with clean ones. Transmission of the coronavirus is mostly by viral droplets on surfaces, including garments, so proper waste management is vital.
In mass living spaces, facilities and circulation routes must also be kept clean and visitors, such as delivery personnel, cleaners, must observe appropriate measures. Frequent disinfection of lift cars, handrails, and keypads is also necessary.
All these considerations to fully prepare hospitals for health crises may mean extra costs. However, in such times when the lives of many depend on proper facilities and services, high capital cost will pay off. Front-liners will be protected, cases can be handled properly, and spread can be minimised.

Makeshift hospitals can be made by reusing existing large spaces such as sport stadiums, warehouses and conference centres; image by Ciao Pederneiras/Shutterstock
EMERGENCY FACILITIES: ADAPTIVE REUSE OF EXISTING LARGE SPACES
Pop-up hospitals have emerged as an alternative to providing additional beds during this crisis. Tents and portable prefabricated modular units based on tried and proven mobile military hospital models have proven effective, but these are not ideal solutions for both healthcare professionals and patients. Hotels can also serve as quarantine facilities, but the design of their air-conditioning systems will need to be adapted to reduce the transmission of air-borne viruses between rooms and common areas.
Also read: COVID-19: An urgent need for emergency architecture
Adaptation of existing large spaces—such as warehouses, conference centres and even indoor sports stadiums—is a better option to rapidly create additional bed capacity. Apart from installing partitions and medical services into these spaces, there is an opportunity to produce modular ICU and ward rooms, complete with ensuites for installation. Such modular systems can also be deployed to provide accommodation in situations of natural disaster, as well as housing the homeless—which is likely to present itself as a real consequence of the economic impacts of a COVID-19 driven economic recession.
The design of large indoor or covered spaces is usually ideal for conversion during emergencies. The very nature of their function usually facilitates ease of access for the delivery and installation of emergency facilities, adequate power supply, sanitary facilities and air-conditioning (if an enclosed venue). Where containment of a contagious outbreak is necessary, improvements in the air-conditioning systems should be considered to enable a fresh-air intake operation rather than recirculation.
Any buildings that rely on air-conditioning in common areas may need to consider more effective cleaning regimes and air purification options. Natural ventilation or fresh air is preferable to recirculating air conditioning systems.
Also read: Optimising airborne infection control through ventilation design
In an ideal world, these major facilities would have good access to support hospitals in case of emergency at the venue, but in reality, they need to be located where best suits their intended use, be it a convention centre, sports stadium or warehouses. Nevertheless, such large facilities would normally have good transport infrastructure to support their intended use, and good access to healthcare facilities. In case of emergency, such as when patients develop severe symptoms and in need for more intensive treatment, good access to hospitals will save lives.

Tents and portable prefabricated modular units can be a solution, but converting existing large spaces such as warehouses and indoor stadiums into makeshift hospitals is rapid and arguably more effective; image by lev radin/Shutterstock
CASE STUDY: CHINA’S EMERGENCY SHELTER HOSPITALS
The Fangcang shelter hospitals—built in Wuhan to handle COVID-19—are large, temporary hospitals constructed by converting public venues to isolate patients with mild to moderate symptoms. The name Fangcang is the Chinese word for Noah’s Ark. These hospitals can be rapidly established to provide large numbers of beds and appropriate care for patients; and offer emotional and social support to help patients cope with the pandemic.
Research report[1] states that the hospital’s design concept has characteristics that suit the needs for public health emergencies. First, the construction is rapid because the physical infrastructure is ready to use. What was needed is redesigning of interior spaces, and purchasing and installing beds; medical devices; and supplies to support care and sheltered living. The conversion process of the first three Fangcang hospitals in Wuhan was completed in 29 hours, providing 4,000 beds in total.
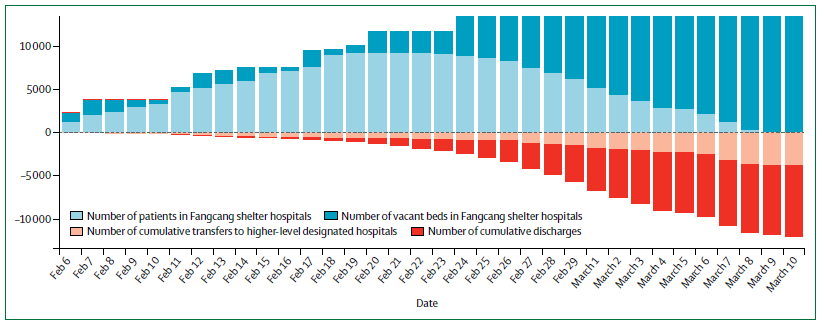
The flows of patients in Fangcang hospitals in Wuhan during the COVID-19 outbreak from February to March 2020. Source: The Lancet
Second, the large-scale public venues, once they have been converted to serve hospital functions, yield massive capacities. In a period of three weeks, China built 16 Fangcang shelter hospitals, providing 13,000 hospitals beds. By 10 March 2020, the hospitals had treated about 12,000 cases. These shelter hospitals took a central part in China’s COVID-19 policy of leaving no patient unattended—sheltering such a large number of people who would otherwise have been quarantined at homes. The large capacities also mean that the hospitals can free up the scarce medical infrastructure of higher-level care, such as the inpatient units providing respiratory support and intensive care.
Third, the building and operations incur lower costs. Conversion avoids costly construction of new physical infrastructure and when the facilities are no longer needed, the structures can be returned to their original purposes, avoiding long-term, inefficient use of space. Operational costs are low because only fewer doctors and nurses are required. This is made possible because all patients share the same primary admission diagnosis and have only mild to moderate symptoms. The uniformity reduced the complexity of care.

Key characteristics and essential functions of Fangcang hospitals. Source: The Lancet
Double-functioning as community centres, the hospitals allowed social engagement to promote patients’ recovery and reduce stress caused by isolation. Being isolated from the COVID-19-negative population might create negative feelings. Health workers provided emotional support and facilitate community activities such as eating together, watching television, dancing, reading, and celebrating birthdays. Of course, such activities adhered strictly to regulations and supervised closely by professionals.
As for residential spaces, a well-designed environment should have a dedicated exercise space, a good landscape, and spaces that help to maintain the dwellers’ mental well-being—all good reasons to engage a good architect, interior designer and landscape architect at the outset.
Temporary shelter hospitals are a definite solution in emergencies, not only for pandemic situations, but in response to natural disasters such as flooding and earthquakes. Rather than adapt the basic functional design of such large public spaces to function as shelter hospitals, there needs to be the ability to install appropriate facilities within these spaces. Portable isolation pods, treatment rooms and even operating theatres can be erected inside such spaces. These modular units are already in use by the military and can be stockpiled for rapid deployment from strategic locations.
INTERGRATED INFRASTRUCTURE PLANNING
In summary, the current global pandemic has reinforced the need for our healthcare facilities to be more adaptable, more resilient, and capable of rapidly increasing capacity to deal with patients requiring a range of support and treatment. It has reminded governments that their countries need to be robust and more self-reliant to cope with such events in the future.
This is not something that private companies or even global companies can address alone, but requires a coordinated approach to best serve the people as we move into a world of diminishing resources and greater environmental challenges.
About the author:

Anton Alers is the founding director of VERITAS Architects Australia and has over 30 years of international architectural experience across a wide range of projects. With over a decade of experience in healthcare and aged care projects, Alers heads the group’s healthcare discipline. He received a master’s degree in architecture from the University of Melbourne in 1991 and is a registered architect in Australia and the UK. He has particular working experience in Australia, the UK, Singapore, Malaysia and Vietnam.
[1] Simiao Chen, Zongjiu Zhang, Juntao Yang, Jian Wang, Xiaohui Zhai, Till Bärnighausen, Chen Wang. 2020. Fangcang shelter hospitals: a novel concept for responding to public health emergencies. Health Policy. https://doi.org/10.1016/S0140-6736(20)30744-3
– Construction+ Online
Disclaimer: Construction+ makes reasonable efforts to present accurate and reliable information on this website, but the information is not intended to provide specific advice about individual legal, business, or other matters, and it is not a substitute for readers’ independent research and evaluation of any issue. If specific legal or other expert advice is required or desired, the services of an appropriate, competent professional should be sought. Construction+ makes no representations of any kind and disclaims all expressed, implied, statutory or other warranties of any kind, including, without limitation, any warranties of accuracy and timeliness of the measures and regulations; and the completeness of the projects mentioned in the articles. All measures, regulations and projects are accurate as of the date of publication; for further information, please refer to the sources cited.
Hyperlinks are not endorsements: Construction+ is in the business of promoting the interests of its readers as a whole and does not promote or endorse references to specific products, services or third-party content providers; nor are such links or references any indication that Construction+ has received specific authorisation to provide these links or references. Rather, the links on this website to other sites are provided solely to acknowledge them as content sources and as a convenient resource to readers of Construction+.






